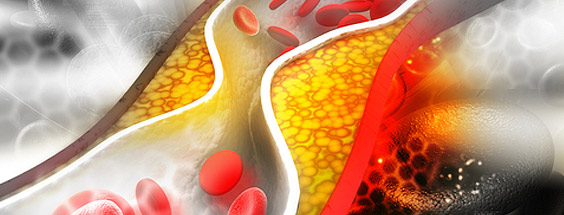
Cholesterol essentially refers to the fats that travel through the arteries and veins, and if they are high enough may get deposited in the vessels (atherosclerosis) and also in tissues contributing to fatty heart, fatty liver, fatty muscle etc.
Cholesterol is composed primarily of 3 main ‘ingredients’. I refer to them as ‘The Good, The Bad, and The UgLy ‘.
The Good cholesterol Is HDL …Think of H as standing for Hoover, and the Higher the better!
The Bad cholesterol is the Triglyceride …
The UgLy cholesterol however is the really Lousy Cholesterol and the Lower the better.
Not everyone needs a tablet.
Sometimes, it’s just a change in your diet that is required and indeed a good diet can reduce your cholesterol by an average of 10%.
A lot depends on your numbers i.e. how much Good, How much Bad and how much Ugly cholesterol you have.
The numbers and targets are also determined by your risks i.e. you rage, if you are a smoker, if you have diabetes, if you have ever had a stroke, if you have a family history etc.
Statins are the number 1 treatment if your Lousy / Ugly / LDL is too high.
There are huge numbers of studies conducted over the last 30 years showing the statins lower LDL cholesterol effectively and significantly reduce your risk for either a first or second heart attack.
Again, your risk assessment determines your personal recommended LDL target (number) and if your level exceeds that, the 1st recommendation would be a statin
If you don’t tolerate your statin, or develop a reaction, there are many ways to tackle this including ad different statin, or a different dose or a different timing schedule. There are other CLASSES of medications, beyond statin that are also well represented in research with proven efficacy and benefit too (just a weaker effect) and they can be tried as alternatives.
Usually, we target the LDL cholesterol at 2.0 and if your doctor has been unable to get to that level, you may need to see an expert who can look at alternative combinations of different drugs to achieve that. There is a new class of drug that has just been launched in the US ( and available in Europe soon ) specifically for people at high risk like you…who either cannot get to target or is unable to take any statin at all.
Absolutely YES.
It is very unusual for men (or women) to have heart attacks at less than aged 50 years. If this happens, it raises the question of a potential genetic disorder one of which is that you make too much cholesterol.
That means that there may be a genetic mutation, and just as your genes may give you read or black ( or brown etc.) hair, your genes can also cause you to make truckloads of cholesterol that gets deposited in the arteries and organs and leave you vulnerable to heart disease. You can very simply (and cheaply) check this out by getting a cholesterol profile, comparing to your Dad and getting an opinion as to whether you might have the disorder.
There is always the possibility you have an undiagnosed condition that predisposed you to make too much cholesterol. Some of these conditions (mutations) are transferred down form father and mother to child, and in some cases the chances are 50/50. So, yes…if your cholesterol is high, and especially if you are young…you should check your child.
This can be done by just measuring cholesterol level opportunistically i.e. when the child is getting a blood test for something else (and you can just tack it on). In children with documented inherited cholesterol disorders, they are started on treatment as young as aged 10 to reduce any risk or burden for heart disease at an early age ( 30’s & 40’s) .
Sometimes it’s not about whether you are fat or thin, active or inactive.
Many people have the person that it is only heavy, inactive people that have high cholesterol and this is a myth. Some people just process too much cholesterol and some people have different risk assessment…and if your cholesterol is high it should be treated.

Diabetes, Endocrinology & Metabolism
